Features
Vital Signs

A conversation with Rice Business Professor Tolga Tezcan on how we can improve hospital operations and payment systems.
Your research mainly focuses on healthcare payment systems and insurance. Can you talk about the history of our national payment systems? How did they come about?
If you look at the early 1900s — when people paid mostly out of pocket — healthcare costs averaged maybe $150 to $200 per year in today’s dollars. Our procedures were not very complicated. They didn’t cost millions or hundreds of thousands of dollars. And people didn’t live as long as they do today. There were many diseases we’ve since learned how to treat.
So, doctors would come to your home. They’d probably give you an aspirin or some kind of antibiotic, and that’s the most they could do. That changed as technology advanced, but our payment system stayed the same until World War II. When people came back from the war, it became clear that a lot of older people could no longer pay for their healthcare.
Private insurance came in and then Medicare and Medicaid in the 1960s. And insurance would pay for your hospital visits. The system had no incentive to be efficient. If insurance is paying, the doctor has no incentive.
Imagine taking your car to a mechanic and saying, “Fix everything.” What kind of bill is that mechanic going to come up with? And that went on until the 1980s when healthcare became more transactional, and costs exploded.
I think we are moving toward a “capitation” payment system. In this system, like what Medicare Advantage does, healthcare institutions will receive a fixed amount — let’s say $10,000. And they’re responsible for everything that relates to an episode of care — let’s say a kneecap replacement. When that happens, now they have all the incentives to keep me healthy. They’re going to encourage me to exercise. They’re going to encourage me not to drink as much, and so on and so forth.
I like the car mechanic analogy. Has the healthcare industry learned a lot from sectors like car manufacturing in terms of how to make their operations more efficient?
Yes. Car manufacturing is the best example.
Some history, again: For whatever reason, the manufacturing sector started using computers a lot earlier than healthcare. Why is that important? Well, by looking at data, you can figure out what the problems in your system are and where the bottlenecks and quality issues are. It’s impossible to do that when everything is handwritten.
The Affordable Care Act changed that. Obamacare was basically the final push to force all hospitals to implement what’s called electronic medical records. If you go to your doctor now, they take notes when they’re talking to you. Sometimes, they have a tablet; they start filling in, checking boxes, and all that. It all goes into a database that we can look at and see how efficient a given clinic is in the first place.
Because of how slowly the healthcare sector adopted digital record-keeping practices, a lot of operational improvements were delayed compared to other manufacturing systems.
Can you share an example of how operational research can make a real difference in healthcare?
There are so many examples I can give you. When I was at the University of Rochester, we were looking at the causes of lengthy treatment times in the emergency room. We had to dig deep into their database to figure out where patients are spending time. From there, we used somewhat standard management tools to understand where the bottlenecks are, and then we’d try to find ways to decrease the hospital’s load.
Emergency rooms, unfortunately nowadays, are anything but emergent unless you’re dying. If you’re dying, they take care of you. Otherwise, you register, and go through triage, usually done by a nurse. The level of triage you fall in kind of determines your priority in the waiting line.
As researchers, we said, “Look: there are so many triage patients coming into the emergency room who could have gone to a primary care physician or to urgent care.” So, we said, “Why don’t we start treatment in triage?” Let’s say you walk in with arm pain. Why don’t we just order an X-ray before you even get to see a doctor? By the time the doctor sees you, the X-rays will be ready — because in the emergency room, doctors and beds are the bottleneck. Not X-rays.
We’re trying to reduce unproductive time. To be clear, I don’t know what is feasible from a medical point of view. Can I even order an X-ray while you’re in the waiting room? I wouldn’t know that.
The people who can come up with these ideas are those who actually work in the system on a daily basis. Our job as researchers is to help healthcare professionals identify these opportunities.
What are some of the biggest hurdles and opportunities we face in Houston, specifically?
As you know, we have a very good city healthcare system — hospitals, universities, medical schools. I don’t think Houston has unique problems that we don’t see elsewhere. The biggest problem, if you ask me, is insufficient insurance coverage. Healthy living in Houston is also a problem.
Otherwise, I think the healthcare system here is in good shape. We have a very good Medicaid system called Harris County Health. There are a lot of initiatives that help the Houston community. But we face the same challenges as other places. Healthcare costs are climbing, and it’s not clear what exactly we can do to stop it.
Imagine taking your car to a mechanic and saying, “Fix everything.” What kind of bill is that mechanic going to come up with? And that went on until the 1980s when healthcare became more transactional, and costs exploded.
Would more of the efficient bottlenecks you’re describing lower overall costs?
Yes, they do somewhat. But the answer to rising healthcare costs is not so simple. In simple economic terms, the healthcare industry has what’s called an “incentive misalignment.” You want to be healthy. And insurance companies want you to be healthy. How do you stay healthy? You go to the gym. You eat healthily. You seek mental services when you need them. But hospitals don’t get paid for these things, and so are currently not incentivized to focus on them.
There’s also a disconnect between healthcare providers. An example: You break your leg, you go to a hospital. They operate on you, and you’re discharged. But then you start physical therapy. And when you’re getting physical therapy, everything depends on what kind of surgery you got, what the doctor decided to do and how the hospital took care of you. If your leg gets worse during therapy instead of better, it could be that the hospital didn’t do the right thing in the first place. But nobody would be penalized for not doing the right thing. Our payment system does not incentivize quality of care.
And from a patient perspective, if the costs of care keep increasing, you’re less likely to see a doctor. Or, if you are informed you’ll need to undergo treatment, you might decide against it, given its cost. And some health-related issues might be a matter of convenience. But if left untreated, a lot of conditions can create other problems down the road, which will magnify the cost of care, in the end.
Much of what you’re saying is specific to the United States. But I’m sure you have a very transnational perspective. You’re a native of Turkiye. You’re speaking with me from London.
Yes, definitely. Whatever you see in America — it’s one system. And there are other ways of doing this. Take the U.K. Until World War II, their system was very similar to the U.S. Obviously, they were more directly impacted by the war. They were bombed all over and lost a lot more people. Their economy got hit really hard. And after the war, they nationalized all the hospitals by running them through “trusts” (i.e., nonprofit organizations). That way, the government can pay hospitals and keep track of quality issues.
There are similarities and differences wherever you go. If you ask me — completely my opinion based on what I’m seeing in healthcare — the U.S. needs to get rid of prices. If Hospital A does a surgery and Hospital B does the same surgery, they should get paid the same amount regardless of insurance. Where they should be competing is on quality. If Hospital A ends up with better surgery outcomes, they should get additional money. And Hospital B should lose some of their money.
The problem in the U.S. is that every insurance company goes around and negotiates with all these hospitals about how they’re going to charge for every single operation. There are thousands of different things that institutions have to negotiate. Compared to the U.K. system, that’s the biggest difference. And that’s where we see the biggest inefficiencies in U.S. healthcare.
Is there anything else you’d like to say about your research? Do you enjoy the work you do?
I’ll say two things. First, healthcare is not just about health. Healthcare is the economy. In strict monetary terms, healthcare keeps everybody healthy so that they can work. We aim to keep young people healthy so they can become adults and contribute. So, when you don’t provide health insurance for people, the whole economy suffers, not just that person’s life.
Even more, if you’re not changing jobs — a job you hate — because you don’t want to lose your health insurance, then you’re not doing a job where you’ll probably be more productive and contribute more to the overall economy. Healthcare is basically the backbone of the economy. So, whenever I hear people say they oppose universal healthcare, I’m just amazed. I can’t really fathom what they’re missing in this.
Second, in terms of research and my personal experience, healthcare operations has been a great field to research. With all due respect to people who research the supply chain, Amazon has billions of dollars to fund research. That’s not the case in healthcare. Healthcare needs people who have the flexibility and training to look at systems and ask systematic questions.
It’s a great area of focus for universities and scholars.
You May Also Like

Features
A third of the world's population is cooking meals over open fires, without access to modern cooking technology. Dymphna van der Lans '02 hopes to change that.

Letter
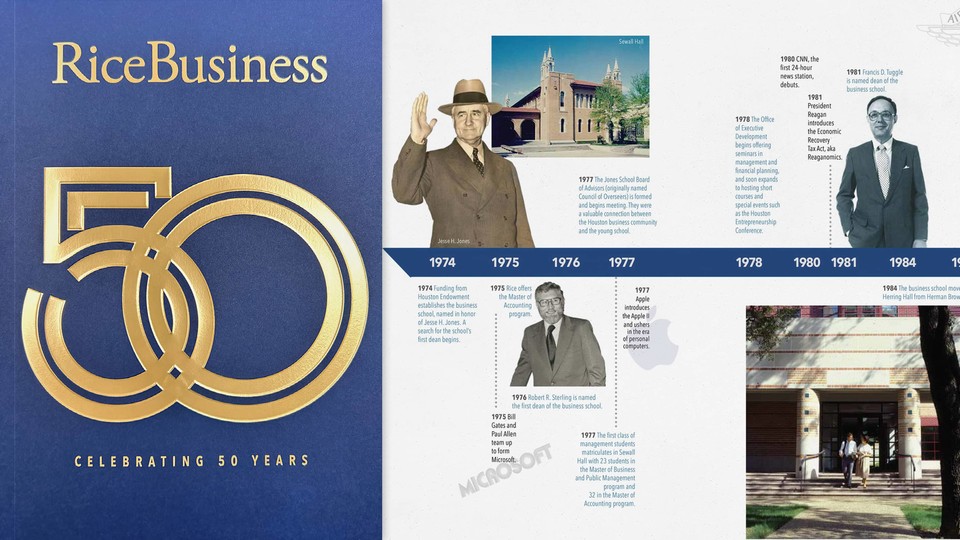
"This year is the perfect time to reflect as we celebrate 50 years since Houston Endowment funded Rice University to establish the business school and reinforce Jesse Jones' legacy to the city."